

NIST Interagency Report
NIST IR 8352
Bitemark Analysis:
A NIST Scientific Foundation Review
Kelly Sauerwein
John M. Butler
Christina Reed
Division 602 - Special Programs Office
Laboratory Programs
National Institute of Standards and Technology
Karen K. Reczek
Division 601 – Standards Coordination Office
Laboratory Programs
National Institute of Standards and Technology
This publication is available free of charge from:
https://doi.org/10.6028/NIST.IR.8352
March 2023
U.S. Department of Commerce
Gina M. Raimondo, Secretary
National Institute of Standards and Technology
Laurie E. Locascio, NIST Director and Under Secretary of Commerce for Standards and Technology

NIST IR 8352
March 2023
Certain commercial entities, equipment, or materials may be identified in this document in order to describe an
experimental procedure or concept adequately. Such identification is not intended to imply recommendation or
endorsement by the National Institute of Standards and Technology, nor is it intended to imply that the entities,
materials, or equipment are necessarily the best available for the purpose.
NIST Technical Series Policies
Copyright, Fair Use, and Licensing Statements
NIST Technical Series Publication Identifier Syntax
Publication History
Approved by the NIST Editorial Review Board on 2022-09-07
How to Cite this NIST Technical Series Publication
Sauerwein K, Butler JM, Reczek KK, Reed C (2023) Bitemark Analysis: A NIST Scientific Foundation Review.
(National Institute of Standards and Technology, Gaithersburg, MD), NIST Interagency Report (IR) NIST IR 8352.
https://doi.org/10.6028/NIST.IR.8352
NIST Author ORCID iDs
Kelly Sauerwein: 0000-0001-9855-3030
John M. Butler: 0000-0001-6472-9157
Karen K. Reczek: 0000-0002-0174-9019
Christina Reed: 0000-0002-4881-1465
NIST IR 8352
March 2023
i
Abstract
This report summarizes a review of the scientific foundations of bitemark analysis conducted by
the National Institute of Standards and Technology (NIST). Bitemark analysis typically involves
examining patterned injuries left on a victim or object at a crime scene, recognizing those
injuries as bitemarks, and comparing those marks with dental impressions from a person of
interest. This review specifically focuses on pattern injuries found on human skin. Over 400
sources were considered via literature searches and input from previous efforts by the National
Institute of Justice Forensic Technology Center of Excellence. Our NIST review also utilized
input from an October 2019 Bitemark Thinkshop organized by the Center for Statistics and
Applications in Forensic Evidence (CSAFE) where experts and stakeholders associated with
bitemark analysis were convened to discuss key issues. Based on this input, our study found a
lack of support for three key premises of the field: 1) human dentition is unique at the individual
level, 2) this uniqueness can be accurately transferred to human skin, and 3) identifying
characteristics can be accurately captured and interpreted by analysis techniques. Furthermore,
our review noted a lack of consensus among practitioners on the interpretation of bitemark data
as well as thoughts on how to move the field forward. If the field seeks to advance, the key
takeaways provided in this review are starting points for areas needing improvement, not an
exhaustive list of specific shortcomings.
Keywords
bitemark; forensic odontology; pattern evidence; dentition; dental morphology; forensic science;
scientific foundation review; interpretation; transference; overlays.

NIST IR 8352
March 2023
ii
Table of Contents
Executive Summary ................................................................................................................ 1
Introduction ...................................................................................................................... 4
Issues Considered and Approaches Taken ................................................................ 5
Limitations ................................................................................................................... 5
Authors and Input Received ........................................................................................ 6
Report Structure .......................................................................................................... 7
Background on Bitemark Analysis ............................................................................... 8
Elements of Bitemark Analysis ................................................................................... 8
2.1.1. Dentition Characteristics ....................................................................................... 8
2.1.2. Challenges with Bitemarks on Skin....................................................................... 9
2.1.3. Available Guidance Documents .......................................................................... 10
Key Areas of Dispute................................................................................................. 11
Data and Information Sources ..................................................................................... 12
Literature Review ...................................................................................................... 12
3.1.1. RTI Literature Review.......................................................................................... 12
3.1.2. NIST Assessment of the Literature ..................................................................... 12
Workshop Discussion (October 2019 CSAFE Bitemark Thinkshop) ....................... 13
Documentary Standards and Guidelines .................................................................. 14
Exploring Factors Influencing Reliability of Bitemark Analysis .............................. 15
Uniqueness of Human Dentition ............................................................................... 15
Transfer and Persistence of Bitemarks ..................................................................... 17
Interpretation of Bitemark Data ................................................................................. 20
4.3.1. Methods of Analysis ............................................................................................ 20
4.3.2. Agreement Among Analysts................................................................................ 22
Conclusions/ Future of Bitemark Analyses ............................................................... 24
Research Needs ........................................................................................................ 24
References ..................................................................................................................... 28
List of Tables
Table 1.1. NIST review team and their areas of expertise……………………………………..
6
Table 1.2. Bitemark Steering Committee members……………………………………….…….
6
Table 2.1. Steps in the evaluation of bitemark data (based on ABFO 2018)………………...10
Table 5.1. Previous statements on lack of scientific foundations for bitemark analysis….….24
NIST IR 8352
March 2023
iii
List of Figures
Figure 1.1. Three key elements of bitemark analysis…………………………….……………..4
Figure 2.1. Illustration of a typical human dental arcade (dentition)………………….………..8
NIST IR 8352
March 2023
iv
Preface
Forensic science plays a vital role in the criminal justice system by providing scientifically based
information through the analysis of physical or digital evidence. The National Institute of
Standards and Technology (NIST) is a non-regulatory scientific research agency within the U.S.
Department of Commerce with a mission to advance measurement science, standards, and
technology. NIST has been working to strengthen forensic science methods for almost a century.
In recent years, several scientific advisory bodies have expressed the need for a review of the
scientific bases of forensic methods and identified NIST as an appropriate agency for conducting
such reviews. A scientific foundation review, also referred to as a technical merit evaluation, is a
study that documents and assesses the foundations of a scientific discipline, that is, the trusted
and established knowledge that supports and underpins the discipline’s methods. Congress has
appropriated funds for NIST to conduct scientific foundation reviews in forensic science. These
reviews seek to answer the question: “What established scientific laws and principles as well as
empirical data exist to support the methods that forensic science practitioners use to analyze
evidence?” Background information on NIST scientific foundation reviews is available in
NISTIR 8225 at https://doi.org/10.6028/NIST.IR.8225.
This report was released for a public comment period from October 11, 2022 to December 12,
2022. In addition, a public webinar was held on October 27, 2022. A total of nine sets of
comments were received including the questions submitted during the webinar. These comments
are available at https://www.nist.gov/spo/forensic-science-program/bitemark-analysis-nist-
scientific-foundation-review. We appreciate the time and thought that went into the comments
and thank the commenters for their suggestions.
Acknowledgments
Richard Cavanagh and Willie May, who have both retired from NIST, provided valuable input
on early efforts with this project. Lynn Garcia from the Texas Forensic Science Commission
supplied input on their previous efforts to assess bitemark evidence. John Morgan, and later
Heidi Eldridge and others, from RTI International provided access to a bitemark literature list
they assembled as part of a separate review. The Center for Statistics and Applications in
Forensic Evidence (CSAFE), a NIST Forensic Science Center of Excellence, organized an
October 2019 Bitemark Thinkshop attended by almost 50 practitioners, researchers, statisticians,
and other stakeholders. We gratefully acknowledge the attendees of this thinkshop and their
contributions to the discussions held there. A summary of this thinkshop, written by Hal Stern
and Alicia Carriquiry along with SNA International contractors, is available at
https://www.nist.gov/forensic-science/scientific-foundation-review-bitemark-analysis
. As with
any field, the scientific process (research, results, publication, additional research, etc.) continues
to lead to advancements and better understanding. Information contained in this report comes
from the authors’ technical and scientific perspectives and review of information available to us
during the time of our study.
NIST IR 8352
March 2023
v
Glossary and Acronyms
AAFS: American Academy of Forensic Sciences
ABFO: American Board of Forensic Odontology
ASFO: American Society of Forensic Odontology
Bitemark: the physical alteration or representative pattern recorded in a medium caused by the contact of
teeth of a human or animal (from ABFO 2018)
Bitemark Analysis: the examination of patterned marks left on a victim or object at a crime scene and
comparing those marks with dental impressions from a person of interest
1
Class Characteristics: features or traits that distinguishes a bitemark from other pattern injuries or
human dentition from non-human dentition patterns
Dental Abrasion: wear on teeth not caused by tooth-on-tooth contact
Dental Arch: arrangement or alignment of maxillary and/or mandibular teeth in the mouth
Dentition: the arrangement of the teeth in the maxillary and mandibular arches
Dental Prothesis: artificial replacement of one or more teeth and structures
Displacement: teeth displaced toward facial/lingual aspect
Forensic Odontology: the use of specialized knowledge in dentistry to assist investigative agencies
Foil: a dentition from an individual that is not a person of interest to be used as a distractor for bitemark
data comparisons.
Individual Characteristics: features or traits that distinguish one person, or their teeth, from any other
IOFOS: International Organization for Forensic Odonto-Stomatology
NRC: National Research Council
Pattern Evidence: markings produced when one object acts upon another object; includes fingerprints,
bitemarks, and toolmarks.
PCAST: President’s Council of Advisors on Science and Technology
Position: location of tooth in the dental arch in relation to others
Rotation: tooth is displaced along its longitudinal axis
Transference: the ability of an object to leave identifying characteristics in material it contacts
1
This report acknowledges that a victim may bite a perpetrator in the course of the attack, however, this report focuses on bites left on a victim
and the process to identify the biter.
NIST IR 8352
March 2023
vi
Wear Pattern: distinctive shape or form of wear on individual teeth
NIST IR 8352
March 2023
1
Executive Summary
All scientific methods have limits and one must understand these limits to use a method
appropriately. This is especially important in forensic science as critical decisions impacting life
and liberty are often based on the results of forensic analyses.
The American Board of Forensic Odontology (ABFO) defines a bitemark as a “physical
alteration or representative pattern recorded in a medium caused by the contact of teeth of a
human or animal.” For human bitemarks, this pattern would demonstrate features, traits, or
characteristics that distinguish the patterned injury as a bitemark (ABFO 2018). Bitemark
analysis typically involves the examination of patterned injuries left on a victim or object at a
crime scene, identification of those injuries as bitemarks, and comparison of those marks with
dental impressions from a person of interest (POI).
The assumption that an individual can be identified from bitemarks left on human skin has, for
several decades, seen a steady increase in scientific scrutiny. In 1960 following an experiment
where multiple people left bitemarks in food items, a British dentist concluded “evidence which
involves the identification of a person by tooth-marks left as bruises in flesh should never be
admitted [in court], and evidence involving bitemarks in, for example, foodstuffs should be
examined extremely critically” (Fearnhead 1960). Unlike the use of dental information to
identify human remains, bitemarks are primarily made from only the anterior teeth and are prone
to distortions due to bite force, location of the bite, and movement of the biter or victim during
the biting event – all of which can lead to an innocent person not being excluded as the source of
a bitemark.
This scientific foundation review examined the existing bitemark literature to answer two
questions: 1) Can bitemarks be accurately associated with teeth that left them? and 2) What data
exist to support or refute this claim in bitemark analysis? The aim of this foundation study is to
promote a better appreciation of the capabilities and limitations of the practice within the
forensic community as well as among other stakeholders, including investigators and legal
professionals. Given the questions already arising from practitioners within this field about the
legitimacy of the fundamental assumptions required to establish a verifiable source of a bitemark
(Avon et al. 2010) and the frequency at which such claims are disproven with DNA testing
(Bowers 2006), this review also focused on the limitations inherent to this practice and under
what conditions they are being observed.
Obtaining input from experts outside of NIST is an integral component of a NIST scientific
foundation review. As described in Chapter 3, the NIST team followed the process outlined in
NISTIR 8225 for conducting this review. This involved:
• collecting and evaluating the peer-reviewed literature,
• assessing publicly available data from interlaboratory studies, proficiency tests, and
laboratory validation studies,
• exploring other available information, including position statements and non-peer
reviewed literature, and obtaining input from members of the relevant community
NIST IR 8352
March 2023
2
through interviews, workshops, working groups, and other formats for the open
exchange of ideas and information.
In addition, this NIST review also sought community input from the 2019 CSAFE Thinkshop
involving practitioners, stakeholders, and researchers. A conclusion from this workshop was that
there is a critical need for research to explore the scientific foundations of bitemark analysis,
including assessing the reliability and validity of determinations made as to bitemark type
(human vs nonhuman vs not a bitemark) and in linking dentition to bitemarks.
It is noted that bitemark analysis represents only a portion of forensic dentistry (odontology)
activities. Antemortem dental records, for example, involving the full human dentition, routinely
enable postmortem identification of human remains. This review does not explore the whole
discipline of forensics odontology; the focus is on bitemarks left on human skin.
Three primary postulates are important for successful bitemark analysis: (1) that dental
characteristics, especially the arrangement of the anterior teeth, differ substantially among
individuals (i.e., uniqueness), (2) skin or other marked surfaces can reliably capture those
differences (i.e., transference), and (3) a bitemark examiner can reliably compare anterior
dentition information with the bitemark image (i.e., interpretation) (Hale 1978, Pretty & Sweet
2001, Saks et al. 2016). This review considers each of these three postulates and finds limited
data to support them. Therefore, the ability of bitemark analysis to accurately exclude or not
exclude individuals as a source of the mark is not supported.
Key takeaways identified as part of this foundation study include the following (numbering is
based on their sequence within the chapter where they are derived):
KEY TAKEAWAY #1.1: Forensic bitemark analysis lacks a sufficient scientific foundation
because the three key premises of the field are not supported by the data. First, human anterior
dental patterns have not been shown to be unique at the individual level. Second, those patterns
are not accurately transferred to human skin consistently. Third, it has not been shown that
defining characteristics of that pattern can be accurately analyzed to exclude or not exclude
individuals as the source of a bitemark.
KEY TAKEAWAY #2.1: The entire human dentition is not represented in a bitemark. Bitemark
patterns typically only represent the anterior teeth and thus not the full possible dentition of an
individual, limiting the amount of information available for an analysis.
KEY TAKEAWAY #4.1: There is a lack of research into population frequencies, specific
identifying characteristics, and measurements that support the notion that human anterior dental
patterns as reflected in bitemarks are unique to individuals.
KEY TAKEAWAY #4.2: Accurate transference of an anterior dentition pattern in the form of a
bitemark on human skin can be limited by distortions caused by skin elasticity, unevenness of the
biting surface, location of the bite, and movement of the biter and/or victim during the biting
event.
NIST IR 8352
March 2023
3
KEY TAKEAWAY #4.3: Comparisons between bitemark patterns made on skin, for example
multiple bitemarks from the same individual on the same victim, have shown that there exists
intra-individual variation in bitemark morphology on the human body such that bitemarks from
the same biter may not appear consistent.
KEY TAKEAWAY #4.4: Bitemarks in cadaver-based research studies are representative of
highly controlled experimental conditions and these results may overestimate the accuracy of
analysis methods. Bitemarks in actual cases, where controlled conditions are not present, are
prone to higher levels of inaccuracy.
KEY TAKEAWAY #4.5: As reflected in research studies to date, bitemark examiners may not
agree on the interpretation of a specific bitemark, including whether the injury is a bitemark, the
features present, and the exclusion or non-exclusion of potential biters.
KEY TAKEAWAY #5.1: Repeated calls for additional data by critics and practitioners (since at
least 1960) suggest insufficient support for the accurate use of bitemark analysis and a lack of
consensus from the community on a way forward.
Calls have been made for empirical studies to assess the limitations of bitemark analysis for
decades. Since 1960, those in the bitemark community have been highlighting the lack of
empirical research and the need to address reliability concerns in bitemark methods. These calls
have largely gone unheeded.
This report describes an examination of publicly available literature and information pertaining
to bitemark analysis. If the field seeks to advance, the key takeaways provided in this report are
starting points for areas needing improvement, not an exhaustive list of specific shortcomings.
NIST IR 8352
March 2023
4
Introduction
When a perpetrator bites a victim, the bitemarks
2
can potentially become evidence of a crime.
Determining that the injury resulted from a human bite, and identifying the source of the mark
(i.e., the biter), requires additional investigation and analysis. The methods used for bitemark
analysis have come under considerable scrutiny and debate.
The questions this scientific foundation review poses include:
(1) Can bitemarks be accurately associated with the teeth that left them?
(2) What data exist to support or refute this claim in bitemark analysis?
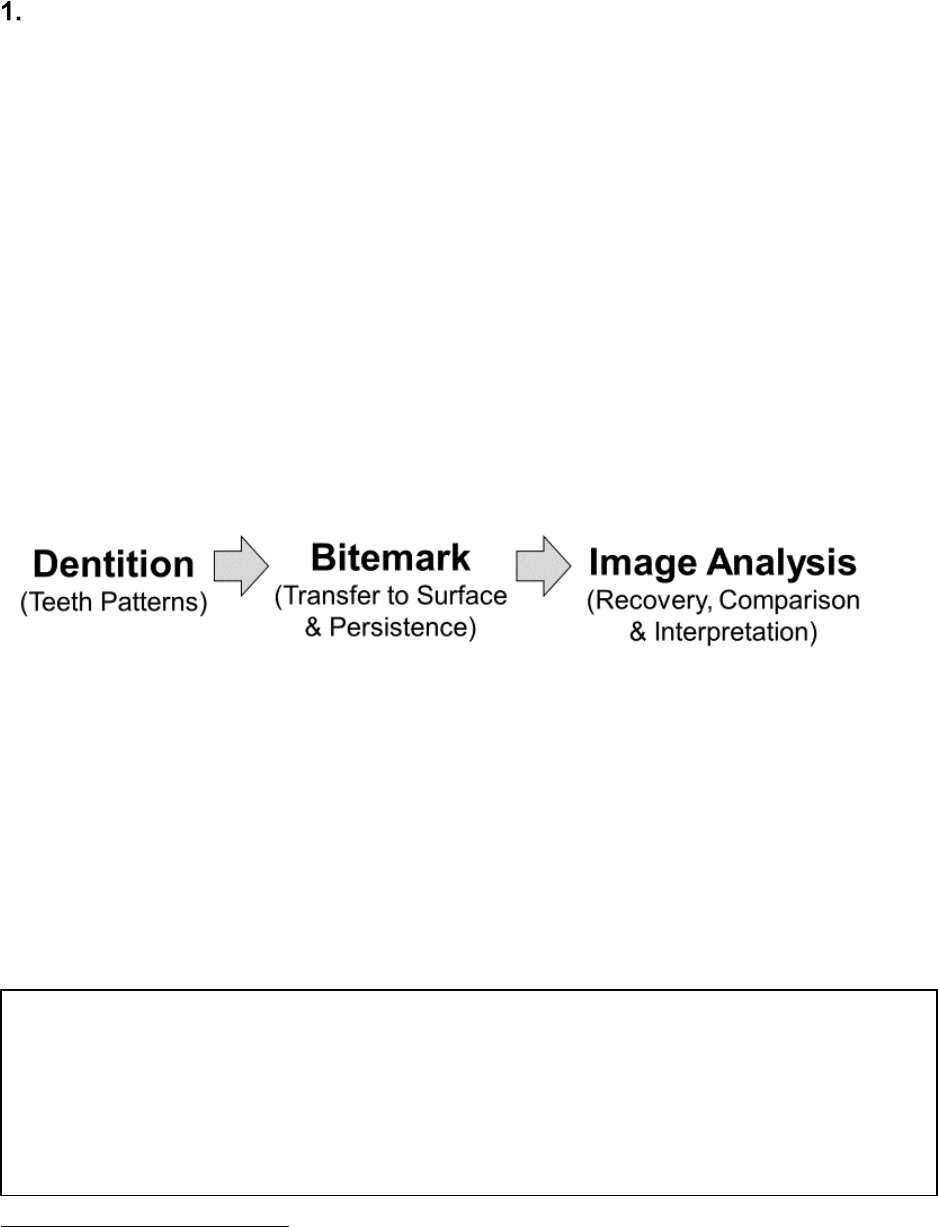
Bitemark analysis typically involves examining patterned injuries left on a victim or object at a
crime scene, recognizing those injuries as bitemarks, and comparing those marks with dental
impressions from a person of interest (POI). Efforts to perform bitemark analysis involve three
key elements (Figure 1.1.): (1) the anterior dentition of the person of interest (the presumed
biter), (2) the accurate transfer of the biter’s dentition to a surface (such as human skin) to
produce a bitemark, and (3) image analysis of the putative bitemark to recover the dental pattern,
compare this pattern to the person of interest’s dentition, and interpret the results.
Figure 1.1. Three key elements of bitemark analysis.
Three primary premises are important for successful bitemark analysis: (1) that dental
characteristics, especially the arrangement of the anterior teeth, differ substantially among
individuals (i.e., uniqueness), (2) skin or other marked surfaces can reliably capture those
differences (i.e., transference), and (3) a bitemark examiner can accurately compare dentition
information with the bitemark image (i.e., interpretation) (Hale 1978, Pretty & Sweet 2001, Saks
et al. 2016). This review found that these three premises are not supported by the data. Therefore,
the ability of bitemark analysis to accurately exclude or not exclude individuals as a source of the
mark is not supported.
2
This report uses the term bitemark or bitemarks as one word rather than two words or as hyphenated words. The singular word usage “is
considered a more progressive term, signifying that odontologists have accumulated a sufficient body of knowledge to dignify the form,”
according to Mark L. Bernstein in chapter 5 of Bitemark Evidence: A Color Atlas and Text, Second Edition (2011), edited by Robert Dorion.
KEY TAKEAWAY #1.1: Forensic bitemark analysis lacks a sufficient scientific
foundation because the three key premises of the field are not supported by the data.
First, human anterior dental patterns have not been shown to be unique at the
individual level. Second, those patterns are not accurately transferred to human skin
consistently. Third, it has not been shown that defining characteristics of that pattern
can be accurately analyzed to exclude or not exclude individuals as the source of a
bitemark.
NIST IR 8352
March 2023
5
This review does not explore the whole discipline of forensic odontology, which includes, for
example, comparing antemortem dental records to postmortem X-rays of the full dentition to
identify human remains. Instead, the focus is primarily on bitemarks left on human skin as they
potentially relate to a crime.
This foundation study on bitemark analysis aims to promote a better appreciation of the
capabilities and limitations of the practice within the forensic community as well as among other
stakeholders, including investigators and legal professionals. Given the questions already arising
from practitioners within this field about the legitimacy of the fundamental assumptions required
to establish a verifiable source of a bitemark (Avon et al. 2010) and the frequency at which such
claims are disproven with DNA testing (Bowers 2006), this review also focused on the
limitations inherent to this practice and under what conditions are they being observed.
Issues Considered and Approaches Taken
A two-day workshop was held in October 2019 with representatives of relevant communities and
stakeholders including odontologists, statisticians, researchers, and lawyers. This event provided
diverse perspectives on the current practices of forensic bitemark analysis and enabled small
group discussions on topics important to scientific foundations of the practice. The full report
from the October 2019 CSAFE Thinkshop is available at
https://doi.org/10.6028/NIST.IR.8352sup1.
A bitemark examiner attempts to exclude or not exclude an individual as being the source of a
bitemark under the premises that (1) human dentition is unique at the individual level, (2) that
uniqueness can be accurately transferred as a bitemark, persist, and be recovered from the
material bitten, and (3) identifying characteristics can be accurately captured and interpreted by
analysis techniques. In other words, bitemark analysis and comparison propose that there are
unique characteristics of human teeth that transfer patterns to bitten surfaces and these
characteristics can be successfully recovered and analyzed to exclude or not exclude individuals
as the source of bitemark.
To assess these issues, we surveyed existing literature in three areas: bitemark analysis on
anterior dental morphology and distinguishing characteristics between individuals, how those
characteristics might transfer and persist in human skin, and empirical studies on the accuracy of
bitemark comparisons, with the goal of identifying the strengths, weaknesses, and knowledge
gaps in the field.
Limitations
A report such as this one provides a snapshot of the current state of the field. Any literature
review, no matter how comprehensive, will be out-of-date as soon as it is published. In addition,
since only published articles or publicly available information and data were sought, some
existing information retained by practitioners may not have been available for review.
The authors of this foundational review are neither lawyers nor forensic odontologists. This
provides an opportunity for a neutral and fresh perspective, but also means that some material
NIST IR 8352
March 2023
6
may have been missed in the review due to inaccessibility. By initially providing this report in
draft form for public comment, we seek input on sources of information that may have been
overlooked.
As with any field, the scientific process (research, results, publication, additional research, etc.)
continues to lead to advancements and better understanding. Information contained in this report
comes from the authors’ technical and scientific perspectives and review of information available
to us during the time of our study. Where our findings identify opportunities for additional
research and improvements to practices, we encourage researchers and practitioners to act to
strengthen methods used to move the field forward.
Authors and Input Received
The review team consisted of four individuals from the National Institute of Standards and
Technology (NIST) whose diverse expertise permitted examination of issues from many
perspectives including lessons learned in other fields. Table 1.1. lists members of the review
team, their NIST operating unit, and their expertise.
Table 1.1. NIST review team and their areas of expertise.
Name NIST Operating Unit Areas of Expertise
John M. Butler Special Programs Office
Forensic DNA, scientific literature, and
research
Karen K. Reczek Standards Coordination Office Documentary standards
Christina Reed Special Programs Office Communications and science writing
Kelly Sauerwein Special Programs Office Biological anthropology
Assistance in finalizing this report was also provided by several additional NIST employees or
contractors as noted in the Acknowledgments. Members of the bitemark analysis community and
various stakeholders provided important input as part of a steering committee (Table 1.2.) that
organized the two-day Bitemark Thinkshop.
Table 1.2. Bitemark Steering Committee (listed in alphabetical order) that met via teleconference multiple
times in 2018 and 2019 to plan the Bitemark Thinkshop held in October 2019.
Name Affiliation Role
Robert Barsley Louisiana State University Odontologist
Mary Bush University of Buffalo Odontologist
John Butler NIST Special Programs Office Researcher

NIST IR 8352
March 2023
7
Name Affiliation Role
Alicia Carriquiry Iowa State University Statistician
Rich Cavanagh NIST Special Programs Office Researcher
Bonner Denton University of Arizona Researcher
Barbara Hervey Texas Court of Criminal Appeals Judge
Donna Kimball NIST Special Programs Office Logistics
Gerald LaPorte
Florida International University
(previously National Institute of Justice)
Researcher
Bill MacCrehan NIST Chemical Sciences Division Researcher
Willie E. May
Morgan State University
(former NIST Director)
Researcher
John Morgan RTI International Researcher
Christopher Plourd Imperial County Superior Court Judge
Rich Press NIST Public Affairs Office Communications
Karen K. Reczek NIST Standards Coordination Office Standards
Hal Stern University of California – Irvine Statistician
Richard
Vorder Bruegge
FBI Laboratory & OSAC Forensic
Science Standards Board (FSSB)
Researcher & Practitioner
Isiah Warner Louisiana State University Researcher
Report Structure
This report contains five chapters. Following this introductory chapter, Chapter 2 provides
background information on bitemarks and describes the principles and practices involved in
bitemark analysis and comparison. Chapter 3 lists the data sources used and how they were
located. Chapter 4 discusses important aspects that influence the accuracy of bitemark data.
Chapter 5 provides conclusions and thoughts on future directions for the field.
Supplemental information to this report is also available at https://www.nist.gov/forensic-
science/scientific-foundation-review-bitemark-analysis. This material includes the full report of
the 2019 CSAFE Bitemark Thinkshop, available standards and guidelines for forensic
odontology, a brief history of public criticisms of bitemark analysis, and the full reference list of
publications examined as part of this study.
NIST IR 8352
March 2023
8
Background on Bitemark Analysis
Elements of Bitemark Analysis
2.1.1. Dentition Characteristics
The American Board of Forensic Odontology (ABFO) defines a bitemark as a “physical
alteration or representative pattern recorded in a medium caused by the contact of teeth of a
human or animal.” For human bitemarks, this pattern would demonstrate features, traits, or
characteristics that distinguish the patterned injury as a bitemark (ABFO 2018). Included in these
class characteristics are measures of size and shape, arrangement, wear and tear, damage, age,
quality, number of individual teeth, prostheses, and replacements (Levine 1977, Verma et al.
2013). During the comparison of a dental impression from a possible suspect with the bitemark
pattern under investigation, several factors are examined including indentations, chips, abrasions,
striations, distances between cusps, tooth width and thickness, alignment, and mouth arch (van
der Velden et al. 2010, Verma et al. 2013).
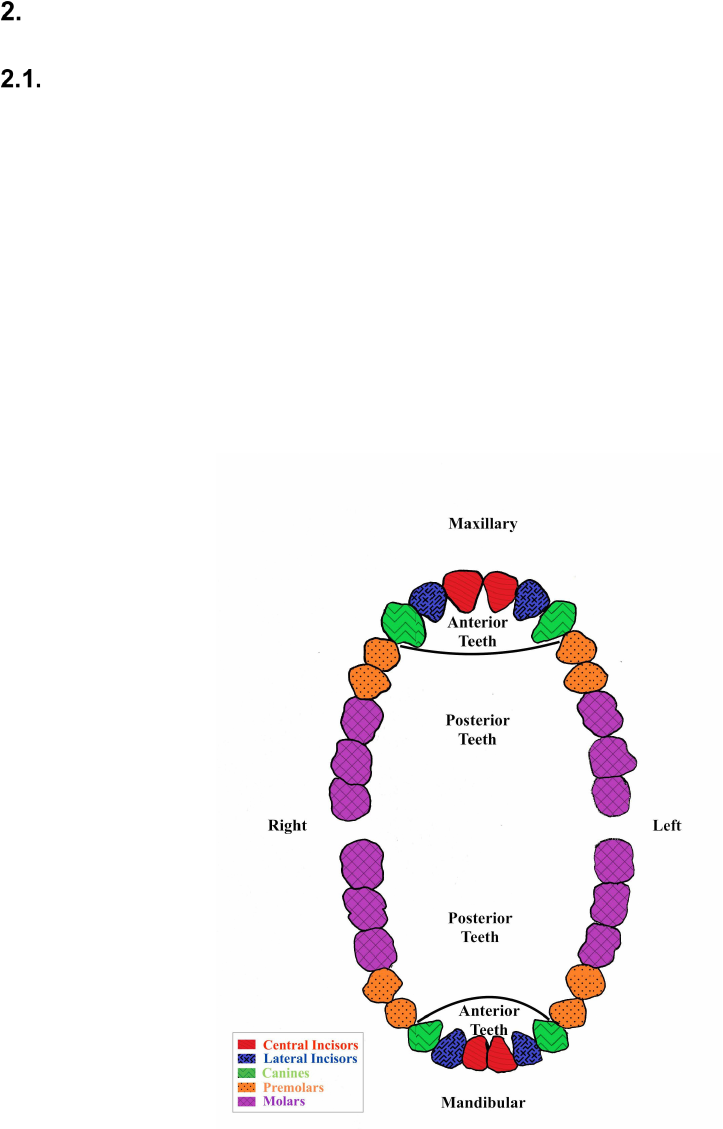
Figure 2.1. Illustration of a typical human dentition viewed in standard anatomical position.
Each tooth type in the human dental arcade has class characteristics that differentiate one type
from the others. The anterior teeth, including central and lateral incisors and canines, are most

NIST IR 8352
March 2023
9
often involved in a bitemark (Figure 2.1.). Bitemark characteristics aid in determining which
marks were made from maxillary or mandibular teeth. Missing teeth, tooth injuries, breakages, or
something obstructing a tooth from the biting surface can account for gaps seen in bitemarks
(Sweet & Pretty 2001).
Individual characteristics are features or traits that distinguish one person, or their teeth, from any
other
. Examples of individual characteristics are those found in the arch (shape, size, tooth
displacement rotation, or drift) and individual teeth (wear pattern, chips, notches, fractures, or
other anomalies).
2.1.2. Challenges with Bitemarks on Skin
According to the ABFO (2018), bitemark data has been utilized to document aspects of violence,
provide a potential link between victim and perpetrator, and help support or refute the history of
events reported or discovered in a legal context. The distortions, elasticity, and evenness of the
surface of the object bitten factor into whether a bitemark is produced and can be accurately
analyzed considering the distortions, elasticity, and evenness of the specific biting surface. In
food or compressible objects other than skin, the pattern is more often visible as a result of tooth
indentations or impressions and occurs with sometimes little force exerted by the biter (e.g.,
bitemarks left in Styrofoam, wax, or cheese).
On skin, the pattern is seen as a vital response to the injury through swelling, scraping (abrasion),
bruising (contusion), or tearing (laceration). Depending on the force of the bite and the skin
itself, the tissue may not show a response and therefore some bites may not leave a mark
(Bernstein 2011).
In addition, human skin can change the appearance of a bitemark over time depending on the rate
and amount of swelling at the site, healing, and skin elasticity; location of the bitemark can
exacerbate these factors and lead to greater distortions (Pretty & Sweet 2001, Vilborn & Bernitz
2021). According to Mark L. Bernstein of the University of Louisville School of Dentistry:
“Bleeding or scraping of skin under assault are not obliged to conform precisely to the anatomy
of the object that produced it” (Bernstein 2011). In this way, human skin as a dependable
material for bitemarks is a key area of dispute in the field.
KEY TAKEAWAY #2.1: The entire human dentition is not represented in a
bitemark. Bitemark patterns typically only represent the anterior teeth and thus not
the full possible dentition of an individual, limiting the amount of information
available for an analysis.
NIST IR 8352
March 2023
10
2.1.3. Available Guidance Documents
The American Board of Forensic Odontologists (ABFO) updated their guidelines in 2018 for
collecting and evaluating bitemark data from both victims and alleged biters. These steps are
summarized in Table 2.1. An evaluation of bitemark data includes:
(1) Examination of questioned pattern to determine whether it is a bitemark
(2) Interpretation and analysis of bitemark features
(3) Comparison of bitemark data to that of POIs and foil (i.e., non-POIs) dentitions
(4) Formation of opinions, if possible, on whether subject and foil dentitions can be excluded
or not excluded as the cause of the bitemark pattern
Table 2.1. Steps in the evaluation of bitemark data (based on ABFO 2018).
Evaluation
Procedure
Determination of
Pattern as Bitemark
Take photographs of mark, including its location and size
Identify mandibular/maxillary arches and midline
Determine whether visible marks caused by individual teeth are
identifiable
Determine whether size/shape of arch is comparable to normal
human variation
Interpretation and
Analysis of Bitemark
Features
Locate pattern and identify features, (e.g., size, shape, anomalies)
Take photographs establishing location and features
Swab for biological evidence
Take impressions of bitemark and victim’s dentition to be turned into
casts for further assessment
Bitemark Comparison
Methods
Generate overlays, including hollow volume, solid volume,
semitransparent representations; computer-generated 2D/3D scans of
subject dentition, 2D photographs of teeth or casts, or 2D/3D scans
of casts
Collect test bites in medium that may include dental wax, animal or
human skin, or other media. Test bites can be used to create overlays
Additional methods - transillumination, computer enhancement
and/or digitization of the mark or teeth, stereomicroscopy, scanning
electron microscopy (SEM), video superimposition, and histology
Formation of
Conclusions
(Levels of Certainty)
Exclude as having made the bitemark
Not exclude as having made the bitemark
Inconclusive
Terms indicating “match” or unconditional linkage to a single
dentition are not sanctioned by ABFO
Of note is the terminology ABFO established limiting the level of certainty an analyst can
conclude from their evaluation of a bitemark and the suspected dentition involved in making that
mark. No dentition is considered as the cause of or a match per se to a specific bitemark. The
language used in this AFBO 2018 document, excluded, not excluded, or inconclusive, indicates a
general sense of uncertainty with any of these conclusions.
NIST IR 8352
March 2023
11
Key Areas of Dispute
Reliability over the following aspects of bitemark analysis remain key areas of dispute: human
skin as an accurate registration material for bitemarks, the uniqueness of human dentition, and
analysis techniques and conclusions.
The ABFO guidelines for bitemark analysis, first published in 1986, have been an attempt to
standardize the collection and analysis of bitemark data. A previous review of bitemark analysis
(NRC 2009) noted disagreement amongst odontologists about standards for comparison and that
usage of these guidelines is voluntary. Additional information related to published criticisms of
forensic odontology and responses to them by odontologists is available at
https://doi.org/10.6028/NIST.IR.8352sup3.
A 2003 study documented adherence to the 1997 version of the ABFO guidelines (McNamee &
Sweet 2003). While practitioners were generally compliant with evidence collection procedures
advocated in the ABFO guidelines, the areas of photographic documentation as well as
impression and excision of the bitemark site lacked consistent adherence and were susceptible to
personal preferences of the examiner. As of early 2022, there has been no recent information
about adherence to the current 2018 ABFO guidelines, so it is unknown whether these past issues
have improved.
NIST IR 8352
March 2023
12
Data and Information Sources
To assess accuracy and other relevant issues related to bitemark analysis and comparison,
empirical data and information were sought from publicly available sources including peer-
reviewed scientific publications, documentary standards, and guidelines.
The NIST Special Programs Office requested the Center for Statistics and Applications in
Forensic Evidence (CSAFE), a NIST Forensic Science Center of Excellence, to organize a
Bitemark Thinkshop in October 2019 to gather input from the community and its stakeholders.
In addition, RTI International (Raleigh, NC), which currently serves as the National Institute of
Justice (NIJ) Forensic Technology Center of Excellence
3
, provided a list of bitemark analysis
articles they considered under a separate systematic review of bitemark data in criminal matters.
Literature Review
Literature – including peer-reviewed publications, reports, and books–was compiled from a
variety of sources described below. These resources primarily addressed the key assumptions of
bitemark analysis: uniqueness, transference, and interpretation.
3.1.1. RTI Literature Review
The NIJ Forensic Technology Center of Excellence within RTI International began a systematic
review of the bitemark literature in 2018. In consultation with leading bitemark practitioners and
researchers, RTI compiled a list of over 100 peer-reviewed journal articles determined to be
relevant to their assessment of the bitemark literature. In November 2019, RTI provided an initial
version of their list to NIST – consisting of the title, reference, and abstract for each article
evaluated. An updated list was provided in April 2021.
3.1.2. NIST Assessment of the Literature
The list provided to NIST from RTI International was compared to the ABFO 2011 annotated
bibliography that was submitted in response to a request by the Subcommittee on Forensic
Science (Butler 2015), as well as a 2011 annotated bibliography compiled by Mary Bush, Peter
Bush, and Iain Pretty (TXFSC 2016). These annotated bibliographies consisted of peer-reviewed
original research papers, review articles, and books. NIST conducted an additional literature
search covering the years of 2010 through 2021. After duplicate references were eliminated, a
total of 403 unique bitemark references remained. The full reference list is available as
supplemental document at https://doi.org/10.6028/NIST.IR.8352sup4
.
Articles examined came from the following journals: Journal of Forensic Sciences, Forensic
Science International, Journal of Forensic Odontostomology, Journal of Forensic Identification,
Journal of the Forensic Science Society, Science & Justice, Journal of Visual Communication in
Medicine, International Journal of Legal Medicine, Research Journal of Medical Sciences,
Journal of the American Dental Association, and the American Journal of Forensic Medicine
and Pathology.
3
See https://forensiccoe.org/
NIST IR 8352
March 2023
13
Sources were evaluated based on their applicability to one of the underlying assumptions of
bitemark analysis – uniqueness, transference, or interpretation – and their use of empirical
methods to assess these assumptions. Sources with empirical data were given priority over case
reports, commentary, legal reviews, opinion pieces, and other similar publications.
Workshop Discussion (October 2019 CSAFE Bitemark Thinkshop)
At the start of this NIST scientific foundation study on bitemark analysis, a workshop was
envisioned as the most effective means of bringing various stakeholders together to discuss
current perspectives on issues. Rich Cavanagh and Karen Reczek of NIST formed an 18-member
steering committee (see Table 1.2.) composed of NIST staff and external stakeholders who met
multiple times via teleconferencing from Spring 2018 until Summer 2019 to plan the event.
Early in the process, the steering committee decided on organizing a thinkshop rather than a
workshop. A workshop involves a brief intensive educational program for a relatively small
group of people that focuses especially on techniques and skills in a particular field, while a
thinkshop is more exploratory and focuses on open challenges and knowledge gaps. The steering
committee selected the invited participants and introductory speakers, defined the meeting
format, and decided on topics for discussion.
The Center for Statistics and Applications in Forensic Evidence (CSAFE)
4
was engaged through
a NIST grant to execute the thinkshop. NIST contracted with SNA International to serve as
breakout session facilitators and meeting notetakers. Invited participants represented a cross-
section of individuals working in forensic odontology and other disciplines and included:
forensic image experts, measurement scientists and researchers, forensic scientists, legal experts
such as prosecutors, defense attorneys and victim advocacy groups, and statisticians. Forensic
odontologists with differing views on the use of bitemark data were actively sought.
The meeting was held over two days in October 2019. The full thinkshop report, which CSAFE
and SNA International provided to NIST, is available at
https://doi.org/10.6028/NIST.IR.8352sup1.
Day one began with six speakers providing introductory remarks to the entire group. Participants
were then divided into three groups of 12 to 15 individuals to discuss one of three specific
questions (Box 3.1). The composition of each discussion group was shuffled over the two-day
event to maximize exposure to different perspectives. During the meeting everyone had an
opportunity to discuss every question. At the end of each breakout session, the entire group
reconvened to hear a summary of what had been discussed in each discussion group. The
thinkshop concluded with all participants gathering for a moderated discussion on conclusions,
takeaways, and next steps.
4
See https://forensicstats.org/
NIST IR 8352
March 2023
14
Documentary Standards and Guidelines
In the area of bitemark analysis, the American Board of Forensic Odontology (ABFO) has
developed and published the ABFO Standards and Guidelines for Evaluating Bitemarks (ABFO
2018). The process used to develop this ABFO document is not known.
In odontology there are several standards developing organizations (SDOs) that are developing,
and publishing standards related to forensic odontology, but not necessarily to bitemark analysis
specifically. Newer standards being developed are using the terms “suspected pattern injury or
patterns produced by human dentition” in lieu of the term “bitemarks.” Additional information
related to available standards in odontology is available at https://doi.org/10.6028/
NIST.IR.8352sup2.
Box 3.1 Bitemark Thinkshop Science Questions
Science Topic #1 (Dentition): Are there measurable characteristics or features in human
dentition that vary among individuals and are persistent within an individual?
Claim: Characteristics of human dentition are unique or can be divided into reliable
fractions of the population, provided consideration of any changes with morphometric
parameters over time and events.
Focus Area A: What measurement method(s) provide the best information for capturing
reliable information about the dentition? Focus Area B: How do we appropriately collect
information to create population databases that can be used for scientific and statistical
analysis of human dentition? Focus Area C: What are the most probative
features/parameters to use, and what are the limits associated with each?
Science Topic #2 (Bitemarks): Do bitemarks transfer measurable characteristics of the
dentition to the substrate?
Claim: Bitemarks in human skin and other substrates reliably reflect the features of
dentition.
Focus Area A: What imaging and measurement method(s) provide the best information
for capturing reliable and reproducible information about the bitemark? Focus Area B:
What contributes to the variability in bitemarks from dentition, and how can the
variability be determined? Focus Area C: What data collection techniques are sufficient
to collect evidence of pattern injuries on human skin?
Science Topic #3 (Analysis and Interpretation): What interpretation strategies
(techniques and practices) produce the most accurate and reliable results?
Claim: Selected data interpretation strategies produce more reliable/defensible results.
Focus Area A: What defines sufficiency to establish reliability in the association of
bitemarks to dentition? Focus Area B: What other data are relevant to bitemark
examination and analysis? Focus Area C: What are the key approaches to take in
bitemark analysis that will ensure the comparison is objective and, if the dentition is not
excluded, the significance of an association is accurately reported?
NIST IR 8352
March 2023
15
Exploring Factors Influencing Reliability of Bitemark Analysis
As discussed in Chapter 2, three primary postulates are important for successful bitemark
analysis: (1) that dental characteristics, especially the arrangement of the anterior teeth, differ
substantially among individuals (i.e., uniqueness), (2) skin or other marked surfaces can
accurately capture those distinctions (i.e., transference), and (3) a bitemark examiner can
accurately compare dentition information with the bitemark image (i.e., interpretation) (Hale
1978, Pretty & Sweet 2001, Saks et al. 2016) to exclude or not exclude POIs.
In each section below, a brief review of the literature of findings on the topics of uniqueness,
transference, and interpretation is provided as well as a summary of observations on those
specific topics from the 2019 Thinkshop (CSAFE 2019). The Key Takeaways highlight
important findings and observations.
Uniqueness of Human Dentition
The premise that every individual’s dentition is unique is fundamental to the process of
comparing a person of interest’s (POIs) dentition with a bitemark pattern found on a victim. Yet
examination of uniqueness and the null hypothesis that another person with similar dentition
could provide an equally plausible bitemark, has produced conflicting results. In addition, only
the anterior teeth of an individual’s dentition are typically involved in creating a bitemark (see
Section 2.1.1), so the full dentition is not usually included in the comparison.
This concept of uniqueness is a strong point used in the analysis of bitemark data to convince
courts that the dentition of one individual is different from other individuals (e.g., Verma et al.
2013, Martin-de-las-Heras et al. 2005) with some comparing dentition to fingerprints or DNA
(Rawson et al. 1984, Verma et al. 2013). However, uniqueness has remained a controversial
point among practitioners. Critics note disagreements on the specific characteristics needed to
establish dental uniqueness and that existing population frequencies of basic tooth measurements
overlap and do not permit identification at the individual level (Brothwell 1963, Keister 1990,
Hillson 1996, Saks et al. 2016, CSAFE 2019).
In 1960, Ron W. Fearnhead of the Departments of Anatomy and Dental Histology at the London
Hospital Medical College conducted a study to examine the match accuracy between dental
models and their corresponding bitemarks made in foods such as cheese, apples, and chocolate as
well as to determine whether two models could ever match the same bitemark. He found that not
only could he correctly match the models of teeth to their corresponding bitemarks, but he also
identified a separate dental model, not associated with the initial study or any of the bitemarks,
that matched the marks “just as perfectly as the models of the jaws that made them” (Fearnhead
1960). This study highlighted the need for more training and research into the forensic
odontology to prevent the community from “the danger of accepting, too readily, evidence which
at first sight appears to be based on an exact science” (Fearnhead 1960).
One of the most frequently cited studies that purported to support the uniqueness of human
dentition utilized computer comparisons of the dental patterns of monozygotic twins (Sognnaes
et al. 1982). This study stated that there were differences in tooth measurements between twins
and bilateral asymmetry within individuals. That is, within twins, the anterior teeth did not reach
NIST IR 8352
March 2023
16
the same horizontal plane at the incisal edges. However, Sognnaes and colleagues only studied
five pairs of twins and while they used a computer-based overlay to compare each twin to the
other, the authors did not provide any quantitative measures of similarity or error (Sognnaes et
al. 1982).
Another study (Rawson et al. 1984) investigated statistical probability of two individuals having
the same number of teeth in matching positions. Using 397 radiographs of wax bite cards
provided by dentists in the United States, the authors estimated that the number of possible
combinations of tooth positions in the lower jaw alone is 6.08×10
12
(i.e., 1 in 6 trillion) and it
would only take a match of 5 teeth in order have “confidence that there would be no other set of
teeth capable of producing the same match” (Rawson et al. 1984). However, they do not state
what is meant by ‘confidence’ or how their U.S. sample can be generalized to the world’s
population. They also neither examined the possibility that tooth positions may be correlated
with one another nor did they compare the individual bitemarks with each other to confirm their
conclusions (Rawson et al. 1984). While Rawson’s (1984) findings have been supported by other
research (Bernitz et al. 2006, Kieser et al. 2007) that claim tooth rotation and arch size and shape
are potentially individualizing characteristics, these evaluations systematically lack population
frequencies and details on measurement bias that may impact their conclusions.
A 2011 study (Bush et al. 2011a) reproduced the statistical analysis Rawson made in 1984 and
found a nonuniform distribution of tooth position within human dentition and concluded that
inferences about the uniqueness of human dentition with purposes for bitemark analysis are not
supported. The 2011 study also found that similarities among 3D scans of 344 dental casts
occurred more often than in Rawson’s original findings, casting strong doubt on the 1-in-6
trillion claim (Bush et al. 2011a). Therefore, any claims that the Rawson study establishes
population frequencies for bitemark patterns could be considered premature.
In 2015, a meta-study of over 1,200 articles identified in electronic library database searches
found only four studies claiming results indicating uniqueness and nine other studies that found
positive matches between different dentitions (Franco et al. 2015). This meta-study concluded
that “the uniqueness of human dentition was not scientifically proven” based on the lack of
sample size/power analyses, appropriate statistical methods, 3D data, and intra- and inter-
examiner analyses.
Participants at the 2019 CSAFE Thinkshop weighed in on the question of the uniqueness of
human dentition and they concluded that such a question was no longer relevant to the field
because it is “highly unlikely” that characteristics exist that could be used to define dental
individuality (CSAFE 2019, section 3.1.2.). Furthermore, the 2018 ABFO Standards and
Guidelines do not condone conclusions that “unconditionally link” a bitemark to a specific
dentition (ABFO 2018, section 1-f). Instead, suspect dentitions should be excluded or not
excluded as having made a bitemark. Thinkshop participants did note that the question of
uniqueness may not even be relevant with the use of exclude or not exclude conclusions. As
odontologists are looking to determine the prevalence or rarity of an individual’s dental pattern,
reliable and scientifically based methods are required to reduce the chance of an incidental
association with someone who should be excluded. Understanding the frequency of class and
individual characteristics in a population is necessary to support a conclusion of excluded or not

NIST IR 8352
March 2023
17
excluded. The thinkshop participants also discussed the uniqueness question indirectly when they
identified the need for standard protocols, definitions for dental measurements, databases, and
consensus for what features should be measured to characterize an individual’s dentition
(CSAFE 2019, section 3.1.1. to section 3.1.2.).
Transfer and Persistence of Bitemarks
Bitemark analysis is also based on the assumption that the individual characteristics of the biter’s
anterior dentition will be accurately transferred to the substrate. Several studies have been
conducted utilizing media other than skin, such as wax (Whittaker 1975, Rawson et al. 1984,
Blackwell et al. 2007), Styrofoam (Pretty 2011), cheese (Layton 1966, Ligthelm et al. 1987), and
apples (Rudland 1982, Ligthelm et al. 1987). However, to be able to generalize to cases where
people bite other people, skin as a substrate must be studied experimentally.
Skin deformation substantially distorts the bitemark in such a way that analysts may be unable to
accurately exclude or not exclude a POI. It has been well-documented that bitemarks recorded in
skin have displayed varying degrees of distortion (Sheasby & MacDonald 2001, Bush et al.
2009, Pretty & Sweet 2010, Sheets et al. 2012, Lewis & Marroquin 2015, Dama et al. 2020).
There are many factors that contribute to the degree of distortion present in a bitemark, including
bite force, surface area and alignment of the dentition, tooth sharpness, elasticity of victim’s skin,
movement during the biting event, and the body’s injury response (e.g., swelling, bruising, and
healing) (Bush et al. 2009, Bush et al. 2010b, Miller et al. 2009, Lewis & Marroquin 2015). For
example, in exploring the role of skin elasticity in bitemark distortion, Lewis and Marroquin
(2015) utilized partial tooth dental stamps that were placed on the curve of the shoulders of 40
volunteers who held their arms in 1 of 4 positions – 1) arms by sides/hands on lap, 2) arms
straight out, 3) arms across the chest/hands on opposite shoulders, or 4) hands held behind the
back. Photographs were taken of each mark, and measurements of individual tooth widths and
mesial to distal and intercanine distances were recorded. Overall, Lewis and Marroquin (2015)
found that distortions increased depending on body position. Tooth width and arch width
distortions were as high as 53.8% and 41.9%, respectively. They also found that bitemark
patterns were unpredictable because distortions were not uniform across the dental arches. While
this study is limited to a single location on the body, it suggests that skin elasticity and body
position are critical variables to be considered when examining a bitemark.
Skin’s anatomical makeup includes biomechanical properties that make skin pliable and elastic
while having considerable tensile strength and toughness (Jablonski 2013). These viscoelastic
properties influence how the tissue responds to a bite.
Studies on bite forces, skin elasticity, and mark distortion document changes in flattening or
constriction of the arch, rotation or displacement of teeth, significant deviation in overall
alignment, the appearance of a missing tooth or diastema although none is present in the source
KEY TAKEAWAY #4.1: There is a lack of research into population frequencies,
specific identifying characteristics, and measurements that support the notion that
human anterior dental patterns as reflected in bitemarks are unique to individuals.
NIST IR 8352
March 2023
18
dentition, mesial-distal width, angles of rotation, and intercanine widths depending on the
tightness of the skin at the time the bite occurs (Bush et al. 2010b, Lewis & Marroquin 2015,
Dama et al. 2020). This is because skin’s properties are based on lines of tension that describe
the magnitude of the stress placed on the skin. In the direction parallel to skin tension, tissue is
inherently tighter, while perpendicular to skin tension, the tissue is looser. The degree and
direction of tension differs according to the location on the body, body movement, and position
(DeVore 1971, Sheasby & MacDonald 2001, Bush et al. 2009, Dama et al. 2020).
One study indicated that firmer tissues such as skin over muscle respond differently when bitten
than skin that was looser or covered fatty tissues (Bush et al. 2009). Another study showed that
all bitemarks used in their research showed some degree of distortion, especially regarding arch
width, which had “extensive and unpredictable” distortions (Sheets et al. 2012).
In addition, Mary Bush and colleagues (Bush et al. 2009) found that multiple bites from a single
dentition showed significant distortions such that no two bitemarks appeared the same. If
bitemarks with the same dentition display such significant distortions that they are not
reproducible from simulated bite to bite, this raises concerns about the accuracy of bitemark
analysis in general and more specifically, the probability that an innocent person can be
accurately excluded as the source of a bitemark.
During the 2019 Bitemark Thinkshop, discussion regarding transfer and persistence of bitemarks
focused on marks made on skin; no other material was discussed. Participants concluded that a
bitemark impression in skin would not record sufficient detail to make an identification at an
individual level and that current imaging methods do not capture all characteristics necessary for
bitemark analysis as these methods cannot determine the force of the bite, bruising depth, or
movement during the bite (CSAFE 2019, sections 4.1.1 - 4.2). Furthermore, they concluded that
fundamental research is needed on how bitemarks are transferred to skin specifically with
attention to identification of the variables that affect bitemark pattern appearance and how skin
may distort the bitemark injury.
Research testing the assumption of accurate transference and persistence of bitemarks has mostly
relied on the use of human cadavers or nonhuman analogues for the biting substrate. For
example, one study examined the accuracy of bitemark comparisons by creating exemplar bites
in pig skin (Whittaker 1975). Aside from ethical concerns related to the use of animals in
KEY TAKEAWAY #4.2: Accurate transference of an anterior dentition pattern in
the form of a bitemark on human skin can be limited by distortions caused by skin
elasticity, unevenness of the biting surface, location of the bite, and movement of
the biter and/or victim during the biting event.
KEY TAKEAWAY #4.3: Comparisons between bitemark patterns made on skin,
for example multiple bitemarks from the same individual on the same victim, have
shown that there exists intra-individual variation in bitemark morphology on the
human body such that bitemarks from the same biter may not appear consistent.

NIST IR 8352
March 2023
19
scientific research, animal skin only partially mimics the features of human skin (Steadman et al.
2018, Dellambra et al. 2019), making generalizations to humans difficult. Pigs are commonly
used in research because their skin is similar to human skin in terms of cell composition,
physiology, and thickness; the biggest difference is a thicker fat layer in pigs (Dellambra et al.
2019). However, as pigs are not humans, researchers need to be careful about generalizing
results found using non-human analogues.
In addition to non-human proxies, numerous studies have utilized cadaver models for bitemark
analysis (Bush et al. 2009, Miller et al. 2009, Bush et al. 2010a, Bush et al. 2010b, Sheets &
Bush 2011, Bush et al. 2011b, Holtkoetter et al. 2013). Because the skin of cadavers loses
elasticity over the postmortem period and does not undergo changes caused by inflammatory
reactions following the bite, it is important to appreciate that the substrate used in the cadaver
research is different than that of a living victim. Marks may not be distorted by movement,
swelling, bruising, or healing. Cadaver-based research employs an unchanging material under
highly controlled conditions and the results may imply a greater accuracy than can be found in
criminally inflicted bites on living individuals. However, those conditions aside, research with
cadaver models has found high levels of variability and incorrect identifications even under these
somewhat controlled conditions. One study found upwards of 16% of foil dentitions could not be
excluded as the biter (Miller et al. 2009), while another found 38% of bitemarks in their sample
showed distortions significant enough where an innocent person might not be excluded as the
biter (Bush et al. 2010a). Bitemarks in actual cases, where those controlled conditions often do
not exist, can be expected to be prone to higher levels of inaccuracy.
The 2019 CSAFE Thinkshop participants repeatedly concluded that fundamental research studies
need to be conducted to identify a standard set of features and measurements to characterize
human bitemarks as well as to determine the resolution needed for imaging the mark. Currently
there is no consensus on what features can be used to accurately determine whether a pattern
injury is a human bitemark (CSAFE 2019, section 4.1.1). Such studies would need to include a
wide range of injuries made in skin on different locations on the body with different degrees of
force, some human-derived, some from animals, and some from other causes. In addition, better
biting devices would be needed to mimic jaw movements (CSAFE 2019, section 4.2). The
attendees at the Thinkshop conceded that it may not be possible to determine all the causal
factors involved in a bitemark under controlled conditions because even in a controlled, well-
planned study, the risk to participants might be too great to obtain institutional review board
(IRB) approval (CSAFE 2019, section 4.1.2).
The findings from animal and cadaver-based research studies demonstrate variability and
indicate that the accurate and consistent transfer of bitemark patterns onto human skin, which is
central to bitemark analysis, is questionable.
KEY TAKEAWAY #4.4: Bitemarks in cadaver-based research studies are representative
of highly controlled experimental conditions and these results may overestimate the
accuracy of analysis methods. Bitemarks in actual cases, where controlled conditions are
not present, are prone to higher levels of inaccuracy.

NIST IR 8352
March 2023
20
Interpretation of Bitemark Data
Once a pattern injury is suspected to be a bitemark, photographs (with appropriate scale) are
taken, and the bitemark is inspected to determine whether there are any identifiable marks
corresponding to maxillary or mandibular arches and/or visible tooth impressions (see Table
2.1.). If those features are present, those marks are then identified as being consistent or not
consistent with human dental morphology (ABFO 2018). After the initial analysis of the
bitemark is completed, if the data is sufficient to conclude a pattern injury is a human bitemark,
comparisons of the bitemark to POIs’ dentitions are conducted. These comparisons can be made
using overlays, either computer or manually generated, test bites, digitization and computer-
aided imaged enhancement, stereomicroscopy, and/or scanning electron microscopy (ABFO
2018). These comparisons may then support a bitemark analyst’s opinion that a POI’s dentition
is excluded as having made the bitemark, not excluded as having made the bitemark, or
inconclusive. These conclusions and all associated data should be included in the analyst’s final
report.
4.3.1. Methods of Analysis
After a pattern injury has been identified as a potential bitemark and data on that mark’s
characteristics has been gathered, analysts use several techniques to identify the injury as a
human bitemark and subsequently exclude or not exclude a dentition as the source of the mark.
4.3.1.1. Overlay Comparisons
Overlays are one method for comparing a POI’s dentition to a bitemark. In a traditional overlay,
the incisal or biting edge of the cast of the POI’s anterior teeth are hand traced onto a transparent
sheet that is then placed over the bitemark or a cast of the bitemark to determine whether they
correspond (McNamee et al. 2005). Some early methods for producing bitemark overlays
included radiographic techniques utilizing metal filings painted into bitemark indentations
(Sognnaes 1977), various photographic techniques (Furness 1968, Havel 1985), tracing the
incisal edges onto an acetate sheet that was then placed over a 1:1 photo of the teeth (Bernstein
1983), and applications involving CAT scans (Rawson 1990) and commercial photocopiers
along with hand-traced perimeters of the teeth (i.e., xerographic methods) (Dailey 1991). Once
the overlay is made, the pattern, size, and shape of the POI’s teeth are compared to the bitemark.
However, some degree of subjectivity is involved in the traditional, hand-traced methods (Sweet
et al. 1998). The accuracy of the overlay can be limited by the quality of the photo, scan, or
photocopy used to create the hand traced outline of the teeth as the individual tooth perimeters
may be difficult to determine. This subjectivity may lead to errors in the overlays which can
make it difficult to reach an accurate conclusion.
Recent advances in digital scanning technology have produced bitemark overlays for
comparisons with POI dentitions, providing a higher-quality image than provided by the hand-
drawn methods. Tai and colleagues (2016) compared the accuracy of bitemark analysis between
three methods: xerographic overlay (e.g., photocopy) with hand tracing, computer-assisted
overlays, and animated superimposition. Based on a 0-3 scoring system where 0 is “totally
unmatched” and 3 is a “definite match,” the animated superimposition method was scored the
highest, meaning that it produced a higher number of probable and definite matches. The
NIST IR 8352
March 2023
21
superimposition method allowed for the comparison of not just the biting edges, but lingual (the
tooth surface closest to the tongue in mandibular teeth) and palatal (the surface closest to the
tongue on maxillary teeth) marking as well (Tai et al. 2016). The xerographic method, however,
was scored the lowest and considered the least accurate and most subjective of the three methods
tested; it required a certain level of examiner expertise to hand-trace the tooth edges and could
not be reproducibly drawn each time a new overlay was generated from the same cast (Tai et al.
2016). The authors did acknowledge that their conditions were ideal because bitemarks were
examined immediately after they were made; no time passed during which the marks could have
faded, and no bruising or other injury occurred that obscured the marks.
A 2017 study supported the findings from Tai et al. (2016) and reported that computer-aided
overlays produced higher-quality images and led to greater accuracy when compared with a cast
dentition than both hand-traced overlays and radiopaque wax impression techniques (i.e., a
radiopaque substance such as zinc oxide eugenol was applied to the individual tooth
impressions) (Pajinagara et al. 2017). In that study, a closed set design was implemented with
only three observers judging overlays of 30 cast dentitions. Those observers had different levels
of experience, with only one being a forensic odontologist, and given the small number of
observers, no generalizations about experience level or accuracy can be made.
Overlay methods used in bitemark analysis to compensate for distortion effects have been shown
to be insufficient and arbitrary as distortions can be nonuniform even within the same bite (Bush
et al. 2010a). Furthermore, the range and magnitude of these distortions differed both between
bites and within each bite making current techniques for compensating for tissue distortion, such
as enlarging or reducing a bitemark photograph, inadequate and unreliable. The risk of
attempting to compensate for nonuniform distortion effects can lead to an innocent person not
being excluded as a POI or the distortion effects being used to explain discrepancies in the mark
to include a POI (Bush et al. 2010a). In both cases, this bias could lead to unsupported inclusions
of innocent individuals.
4.3.1.2. 3D Scans
Because overlays utilize a 2D image of a 3D structure, potentially valuable information can be
lost such as the shape of the dentition, the curvature of the bitten surface, and the depth of tooth
penetration into the bitten object (Giri et al. 2019). Furthermore, since bitemarks undergo
distortion during both the biting event and the healing process that follows, it has been argued
that a scan is a representation of a distorted bitemark (Vilborn & Bernitz 2021). Three-
dimensional digital scanning enables accurate and fast recording of bitemarks made in soft
substances – such as cheese, chocolate, pears, apples, and human skin – without further
distortion of the mark during impression taking (Stols & Bernitz 2010, Naether et al. 2012,
Vilborn & Bernitz 2021). A 3D scanner generates point clouds from geometric data gathered
from the surface of an object and the object’s shape is then reconstructed from the spatial
position of the digital data. Two types of 3D scanners – contact and laser – are utilized in
bitemark analysis. Contact scanners, also known as point-to-point or linear scanners, scan the
surface of an object via a probe and internal sensors determine the spatial positioning of the
probe so 3D reconstruction can be achieved. Laser scanners are non-contact devices that emit a
NIST IR 8352
March 2023
22
laser beam onto an object’s surface and the laser is reflected back to the scanner to reconstruct
the object.
A study comparing the accuracy of contact and laser scanners as measured by uncertainty values
reported no significant differences between the two types of scanners; uncertainty values ranged
from 0.07 mm to 0.39 mm for single linear measurements and upwards of 0.43 mm to 1.15 mm
for intercanine distances (Molina & Martin-de-las-Heras 2015). While these two scanning
technologies performed similarly, each has its own limitations: Contact scanners are unable to
capture surfaces with marked concavity and have a greater potential to inadvertently damage
evidence (Molina & Martin-de-las-Heras 2015, Vilborn & Bernitz 2021). Non-contact methods,
avoid the problem of possibly damaging the evidence as there is no contact between the scanner
and the biting surface. However, they have difficulty detecting sharp edges, especially the incisal
edge of the anterior incisors, leading to incorrect depictions of tooth morphology (Molina &
Martin-de-las-Heras 2015). When using the 3D laser scanners for dental casts and biting edges in
practical forensic cases, these potential sources of error should be considered (Molina & Martin-
de-las-Heras 2015, Vilborn & Bernitz 2021).
4.3.2. Agreement Among Analysts
Multiple studies have demonstrated a widespread lack of agreement on conclusions reached with
bitemark data, including those relating to whether the mark was indeed a bitemark, features
present, and inconsistency in techniques used to analyze bitemarks from one case to the next
(Page et al. 2013, Freeman & Pretty 2015, Reesu & Brown 2016). Freeman and Pretty (2015)
measured the degree of consensus among bitemark analysts using a preliminary decision tree
designed by the ABFO to aid odontologists in their assessment, analysis, and conclusions for
bitemarks. Each analyst answered the following three questions for 100 case photos: 1) Is there
sufficient data to render an opinion on whether the patterned injury is a human bitemark? 2) Is it
a human bitemark, not a human bitemark, or suggestive of a human bitemark? and 3) Does the
bitemark have distinct, identifiable arches and individual tooth marks? Overall, only 8% of cases
achieved 90% agreement across the three questions. While this study only examined agreement
and not accuracy, the lack of agreement among the 39 bitemark analysts casts doubt on the utility
of bitemark analysis as a viable method of excluding or not excluding individuals.
A 2016 study of members of the British Association for Forensic Odontology (BAFO) reported
similar results as Freeman and Pretty (2015) in that disagreement was found not only between
odontologists on whether a patterned injury was a bitemark, whether it was human or animal, or
adult or child, but it also found inconsistency within individual odontologists after reassessing
the marks eight weeks later (Reesu & Brown 2016). This lack of agreement on the basics of
bitemark analysis highlights a fundamental flaw of bitemark analysis methods and casts heavy
doubt on the accuracy of the conclusions of such analysis. Similar conclusions have been
reached for decades (Whittaker 1975, Whittaker et al. 1998, Arheart & Pretty 2001).

NIST IR 8352
March 2023
23
The 2019 CSAFE Bitemark Thinkshop tackled this question and determined that there was not
enough data to establish the degree to which practitioners can reliably associate bitemarks to
individual dentition patterns. They also stressed that practitioners should avoid the term “match”
in their interpretations due to the qualitative and subjective nature of bitemark analysis (CSAFE
2019). This echoes the best practices guidelines put forward in 2018 by the ABFO which caution
that conclusions regarding bitemark linkage should only exclude or not exclude a dentition as
having made the bitemark. Stronger terms regarding matching or conclusive identification are
not condoned by the ABFO or the thinkshop participants.
KEY TAKEAWAY #4.5: As reflected in research studies to date, bitemark
examiners may not agree on the interpretation of a specific bitemark, including
whether the injury is a bitemark, the features present, and the exclusion or non-
exclusion of potential biters.
NIST IR 8352
March 2023
24
Conclusions/ Future of Bitemark Analyses
Research Needs
Calls have been made for empirical studies to assess the limitations of bitemark analysis for
decades. Since 1960, those in the bitemark community have been highlighting the lack of
empirical research and the need to address reliability concerns in bitemark methods (Table 5.1).
These calls have largely gone unheeded.
This report examined publicly available literature and information pertaining to bitemark
analysis. Forensic bitemark analysis lacks a sufficient scientific foundation because the three key
premises of the field are not supported by the data. First, human anterior dental patterns have not
been shown to be unique at the individual level. Second, those patterns are not accurately
transferred to human skin consistently. Third, it has not been shown that defining characteristics
of that pattern can be accurately analyzed to exclude or not exclude individuals as the source of a
bitemark. The data available does not support the accurate use of bitemark analysis to exclude or
not exclude individuals as the source of a bitemark. If the field seeks to advance, the key
takeaways provided in this report are starting points for areas needing improvement, not an
exhaustive list of specific shortcomings.
Table 5.1. Previous statements on lack of scientific foundations for bitemark analysis
#
Reference
Citation
Statement
1
Fearnhead
1960
“Apart from a few isolated places research in forensic odontology
is non-existent…[after discussing results from an experiment he
performed] I do not wish to overstate the importance of this
experiment, but I do hope that it serves to illustrate the need for a
more critical awareness by the legal profession and those concerned
in forensic science of the danger of accepting, too readily, evidence
which at first sight appears to be based on an exact science. This
awareness can only come through the dissemination of knowledge
from the sciences, which, in turn, can only be obtained through
researches.”
"…evidence which involves the identification of a person by tooth-
marks left as bruises in flesh should never be admitted, and
evidence involving bite-marks in, for example, foodstuffs should be
examined extremely critically."
KEY TAKEAWAY #5.1: Repeated calls for additional data by critics and
practitioners (since at least 1960) suggest insufficient support for the accurate use
of bitemark analysis and a lack of consensus from the community on a way
forward.
NIST IR 8352
March 2023
25
#
Reference
Citation
Statement
2 DeVore 1971
“…once the skin has been excised, the shrinkage is so great and so
irregular as to make its value for identification of bite marks
extremely doubtful.”
3
Barbenel &
Evans 1974
"…we are still ignorant of the conditions during normal biting and
hence considerable research is needed into this before simulation
studies can be considered of real clinical and forensic relevance."
4 Rothwell 1995
"There is no consensus on the appropriate technical methods for
evaluating the bite mark and potentially associated dental
composition.”
“Above all, the investigator should recognize the innate problems
in bite mark examination and avoid expanding the analysis beyond
rational boundaries.”
“Forensic dentists need to approach bite marks with a certain
degree of skepticism and continually acknowledge their
limitations.”
5
Pretty &
Sweet 2001
“From this review of the literature, it is possible to state that the
issue of skin distortion in bitemark analysis has not been fully
addressed and the cautions issued by DeVore [see row #2 above in
this table] and others should still be heeded today.”
6 Senn 2007
“…good intentions are no substitute for scientific thoroughness…
Pretty and Sweet’s 2001 words still ring true in 2006…‘Despite the
continued acceptance of bitemark evidence in European, Oceanic
and North American Courts, the fundamental scientific basis for
bitemark analysis has never been established’ (Pretty & Sweet
2001). Although there have been efforts and concern by forensic
odontologists in the area of bite mark analysis, the body of
knowledge verified by research, the demonstratable level of
expertise proven by proficiency testing, and the establishment and
enforcement of standards and ethics are seriously lacking. These
failures are a profound detriment to the professional standing of
forensic odontology.”
“The conclusion by anyone that one person in an open population
can be said to have created a bite pattern on human skin with
reasonable certainty cannot be scientifically supported.” (emphasis
in the original)
7
National
Academy of
Sciences
committee
(NRC 2009)
The scientific basis of these methods was “insufficient to conclude
that bitemark comparisons can result in a conclusive match”
NIST IR 8352
March 2023
26
#
Reference
Citation
Statement
“A standard type, quality, and number of individual characteristics
required to indicate that a bitemark has reached a threshold of
evidentiary value has not been established.”
8
Franco et al.
2015
“Based on the performed systematic review, the uniqueness of
human dentition was not scientifically proven. Specifically, the
lack of (1) a power analysis for the stratification and size
calculation of the studied sample, (2) intra- and inter-examiner
calibrations, (3) advanced 3D data registration, (4) automated
landmarking, (5) validated 3D shape comparison software, and (6)
statistical methods and quantifications for data comparison present
the main limitations in the studies aiming to prove the uniqueness
of human dentition.”
9
Texas
Forensic
Science
Commission
2016
“The Commission recommends that bitemark comparison not be
admitted in criminal cases in Texas unless and until the following
are established: (1) Criteria for identifying when a patterned injury
constitutes a human bitemark. This criteria should be expressed
clearly and accompanied by empirical testing to demonstrate
sufficient inter and intra-examiner reliability and validity when the
criteria are applied…” (emphasis in the original)
10
Reesu &
Brown 2016
“If bite mark analysis is to continue…forensic odontologists would
do well to bolster the research base behind their methodology in
forming opinions on bite marks.”
“There are differences in opinions between forensic odontologists
when considering the same case involving a bite mark.
Furthermore, forensic odontologists as individuals changed their
opinions when looking at the same case after a wash-out
period…Opinions on bite mark evidence should be treated with
caution, further research done, and introduction of a recognized
system for both validation/revalidation.”
11 PCAST 2016
“…bitemark analysis does not meet the scientific standards for
foundational validity, and is far from meeting such standards. To
the contrary, available scientific evidence strongly suggests that
examiners cannot consistently agree on whether an injury is a
human bitemark and cannot identify the source of bitemark with
reasonable accuracy.”
NIST IR 8352
March 2023
27
#
Reference
Citation
Statement
12 Bowers 2019
“…clearly recognize the facts of weak foundational science,
absence of empirical proofs, dependence on group acceptance
as a
substitute for validity, and resulting damaging effects to the
criminal justice system...”
“The tide against its continued use can be summed up in succinct
terms:
• A lack of valid evidence to support many of the
assumptions and assertions made by forensic dentists during
bite-mark comparisons.
• Error rates by forensic dentists are perhaps the highest of
any forensic identification specialty still being practiced.
• Bitemark testimony has been ‘introduced in criminal trials
without any meaningful scientific validation, determination
of error rates, or reliability testing.’”

NIST IR 8352
March 2023
28
References
ABFO (2011) “RDT&E IWG Human Bitemark Analysis Question List” annotated bibliography
provided October 2, 2011, by the American Board of Forensic Odontology to the National
Science and Technology Council’s Subcommittee on Forensic Science Research, Development,
Testing and Evaluation Interagency Working Group. Available at
https://www.nist.gov/system/files/documents/forensics/Annotated-Bibliography-Odontology.pdf.
Accessed September 29, 2022.
[ABFO 2018] American Board of Forensic Odontology (2018) Standards and Guidelines for
Evaluating Bitemarks. Available at https://abfo.org/resources/id-bitemark-guidelines/. Accessed
September 29, 2022.
Arheart KL, Pretty IA (2001) Results of the 4th ABFO Bitemark Workshop--1999. Forensic
Science International 124(2-3):104-111.
Avon SL, Victor C, Mayhall JT, Wood RE (2010) Error rates in bite mark analysis in an in vivo
animal model. Forensic Science International 201(1-3):45-55.
Barbenel JC, Evans JH (1974) Bite marks in skin--mechanical factors. Journal of Forensic
Science Society 14(3):235-238.
Bernitz H, van Heerden WF, Solheim T, Owen JH (2006) A technique to capture, analyze, and
quantify anterior teeth rotations for application in court cases involving tooth marks. Journal of
Forensic Sciences 51(3):624-629.
Bernstein ML (1983) The application of photography in forensic dentistry. Dental Clinics of
North America 27(1):151-170.
Bernstein ML (2011) The nature of bitemarks. In Dorion RBJ (ed.) Bitemark Evidence: A Color
Atlas and Text, Second Edition. Boca Raton: CRC Press, pp. 53-65.
Blackwell SA, Taylor RV, Gordon I, Ogleby CL, Tanijiri T, Yoshino M, Donald MR, Clement
JG (2007) 3-D imaging and quantitative comparison of human dentitions and simulated bite
marks. International Journal of Legal Medicine 121(1):9-17.
Bowers CM (2006) Problem-based analysis of bitemark misidentifications: the role of DNA.
Forensic Science International 159:S104-S109.
Bowers CM (2019) Review of a forensic pseudoscience: Identification of criminals from
bitemark patterns. Journal of Forensic and Legal Medicine 61:34-39.
Brothwell DR (1963) Dental Anthropology, First Edition. Oxford: Pergamon Press.
Bush MA, Miller RG, Bush PJ, Dorion RB (2009) Biomechanical factors in human dermal
bitemarks in a cadaver model. Journal of Forensic Sciences 54(1):167-176.
NIST IR 8352
March 2023
29
Bush MA, Thorsrud K, Miller RG, Dorion RB, Bush PJ (2010a) The response of skin to applied
stress: investigation of bitemark distortion in a cadaver model. Journal of Forensic Sciences
55(1):71-76.
Bush MA, Cooper HI, Dorion RB (2010b) Inquiry into the scientific basis for bitemark profiling
and arbitrary distortion compensation. Journal of Forensic Sciences 55(4):976-983.
Bush MA, Bush PJ, Sheets HD (2011a) Statistical evidence for the similarity of the human
dentition. Journal of Forensic Sciences 56(1):118-123.
Bush MA, Bush PJ, Sheets HD (2011b) A study of multiple bitemarks inflicted in human skin by
a single dentition using geometric morphometric analysis. Forensic Science International 211(1-
3):1-8.
Butler JM (2015) U.S. initiatives to strengthen forensic science & international standards in
forensic DNA. Forensic Science International: Genetics 18:4-20. Available at
https://doi.org/10.1016/j.fsigen.2015.06.008. Accessed September 29, 2022.
[CSAFE 2019] Center for Statistics and Applications in Forensic Evidence, SNA International
(2020). NIST CSAFE Bitemark Thinkshop October 17
th
-18
th
, 2019: Report. Available at
https://www.nist.gov/forensic-science/scientific-foundation-review-bitemark-analysis.
Dailey JC (1991) A practical technique for the fabrication of transparent bite mark overlays.
Journal of Forensic Sciences 36(2):565-570.
Dama N, Forgie A, Mânica S, Revie G (2020) Exploring the degrees of distortion in simulated
human bite marks. International Journal of Legal Medicine 134(3):1043-1049.
Dellambra E, Odorisio T, D’Arcangelo D, Failia CM, Facchiano A (2018) Non-animal models in
dermatological research. ALTEX 36(2): 177-202.
DeVore DT (1971) Bite marks for identification? A preliminary report. Medicine, Science, and
the Law 11(3):144-145.
Dorion RBJ (editor) (2011) Bitemark Evidence: A Color Atlas and Text, Second Edition. CRC
Press: Boca Raton.
Fearnhead RW (1960) Facilities for forensic odontology. Medicine, Science, and the Law 1:273-
277.
Franco A, Willems G, Souza PH, Bekkering GE, Thevissen P (2015) The uniqueness of the
human dentition as forensic evidence: a systematic review on the technological methodology.
International Journal of Legal Medicine 129(6):1277-1283.
Freeman AJ, Pretty I (2015) Construct validity of bitemark assessments using the ABFO
decision tree. Presentation made to the 2015 Annual Meeting of the American Academy of

NIST IR 8352
March 2023
30
Forensic Sciences. Available at:
https://www.wsj.com/public/resources/documents/ConstructValidBMdecisiontreePRETTYFREE
MAN.pdf. Accessed September 29, 2022.
Furness J (1968) A new method for the identification of teeth marks in cases of assault and
homicide. British Dental Journal 124(6): 261-267
Giri S, Tripathi A, Patil R, Khanna V, Singh V (2019) Analysis of bite marks in food stuffs by
CBCT 3D-reconstruction. Journal of Oral Biology and Craniofacial Research 9: 24-27.
Hale A (1978) The admissibility of bite mark evidence. Southern California Law Review
51(2):309-334.
Havel DA (1985) The role of photography in the presentation of bitemark evidence. Journal of
Biological Photography 53(2): 59-62.
Hillson, S (1996) Dental Anthropology. Cambridge, UK: Cambridge University Press.
Holtkötter H, Sheets HD, Bush PJ, Bush MA (2013) Effect of systematic dental shape
modification in bitemarks. Forensic Science International 228(1-3):61-69.
Jablonski NG (2013) Skin: A Natural History. Berkeley: University of California Press, pp.9-20.
Keister, JA (1990) Human Adult Odontometrics – The Study of Variation in Adult Tooth Size.
Cambridge, UK: Cambridge University Press.
Kieser JA, Bernal V, Neil Waddell J, Raju S (2007) The uniqueness of the human anterior
dentition: a geometric morphometric analysis. Journal of Forensic Sciences 52(3):671-677.
Layton JJ (1966) Identification from a bite mark in cheese. Journal of the Forensic Science
Society 6:76-80.
Levine LJ (1977) Bite mark evidence. Dental Clinics of North America 21(1):145-158.
Lewis C, Marroquin LA (2015) Effects of skin elasticity on bite mark distortion. Forensic
Science International 257:293-296.
Ligthelm AJ, Coetzee WJ, van Niekerk PJ (1987) The identification of bitemarks using the reflex
microscope. Journal of Forensic Odontology 5(1): 1-8.
Martin-de-las-Heras S, Valenzuela A, Ogayar C, Valverde AJ, Torres JC (2005) Computer-based
production of comparison overlays from 3D-scanned dental casts for bite mark analysis. Journal
of Forensic Sciences 50(1):127-133.
McNamee AH, Sweet D (2003) Adherence of forensic odontologists to the ABFO guidelines for
victim evidence collection. Journal of Forensic Sciences 48(2):382-385.

NIST IR 8352
March 2023
31
McNamee AH, Sweet D, Pretty I (2005) A comparative reliability analysis of computer-
generated bitemark overlays. Journal of Forensic Sciences 50(2):400-405.
Miller RG, Bush PJ, Dorion RB, Bush MA (2009) Uniqueness of the dentition as impressed in
human skin: a cadaver model. Journal of Forensic Sciences 54(4):909-914.
Molina A, Martin-de-las-Heras S (2015) Accuracy of 3D scanners in tooth mark analysis.
Journal of Forensic Sciences 60(S1):S222-S226.
Naether S, Buck U, Campana L, Breitbeck R, Thali M (2012) The examination and identification
of bite marks in foods using 3D scanning and 3D comparison methods. International Journal of
Legal Medicine 126(1):89-95.
[NISTIR 8225] Butler JM, Iyer H, Press R, Taylor MK, Vallone PM, Willis S (2020) NIST
scientific foundation reviews. NISTIR 8225. Available at https://doi.org/10.6028/NIST.IR.8225.
Accessed September 29, 2022.
[NRC 2009] National Research Council (2009) Strengthening Forensic Science in the United
States: A Path Forward. National Academies Press, Washington, D.C.
Page M, Taylor J, Blenkin M (2013) Expert interpretation of bitemark injuries--a contemporary
qualitative study. Journal of Forensic Sciences 58(3):664-672.
Pajnigara NG, Balpende AS, Motwani MB, Choudhary A, Thakur S, Pajnigara NG (2017) A
comparative study of three commonly used two-dimensional overlay generation methods in bite
mark analysis. Journal of Oral and Maxillofacial Pathology 21:442-446.
[PCAST 2016] President’s Council of Advisors on Science and Technology (PCAST)
(September 20, 2016) Report to the President: Forensic Science in Criminal Courts: Ensuring
Scientific Validity of Feature-Comparison Methods. Available at
https://obamawhitehouse.archives.gov/sites/default/files/microsites/ostp/PCAST/pcast_forensic_
science_report_final.pdf. Accessed September 29, 2022.
Pretty IA, Sweet D (2001) The scientific basis for human bitemark analyses—a critical review.
Science & Justice 41(2):85-92.
Pretty IA, Sweet D (2010) A paradigm shift in the analysis of bitemarks. Forensic Science
International 201:38-44.
Pretty IA (2011) Reliability of bitemark evidence. In: Dorion RBJ (ed). Bitemark Evidence: A
Color Atlas and Text, Second Edition. CRC Press: Boca Raton, pp. 587-599.
Rawson RD, Ommen RK, Kinard G, Johnson J, Yfantis A (1984) Statistical evidence for the
individuality of the human dentition. Journal of Forensic Sciences 29(1):245-253.

NIST IR 8352
March 2023
32
Rawson RD (1990) Production of bite mark overlays from CAT scans and model positioning
apparatus. Proceedings of the American Academy of Forensic Sciences Denver, CO; Publication
Printers, Corp. p.112
Reesu GV, Brown NL (2016) Inconsistency in opinions of forensic odontologists when
considering bite mark evidence. Forensic Science International 266:263-270.
Rothwell BR (1995) Bite marks in forensic dentistry: a review of legal, scientific issues. Journal
of the American Dental Association 126(2): 223-232.
Rudland M (1982) The dimensional stability of bitemarks in apples after long-term storage in a
fixative. Medicine, Science, and the Law 22(1): 47-50.
Saks MJ, Albright T, Bohan TL, Bierer BE, Bowers CM, Bush MA, Bush PJ, Casadevall A,
Cole SA, Denton MB, Diamond SS, Dioso-Villa R, Epstein J, Faigman D, Faigman L, Fienberg
SE, Garrett BL, Giannelli PC, Greely HT, Imwinkelried E, Jamieson A, Kafadar K, Kassirer JP,
Koehler J', Korn D, Mnookin J, Morrison AB, Murphy E, Peerwani N, Peterson JL, Risinger
DM, Sensabaugh GF, Spiegelman C, Stern H, Thompson WC, Wayman JL, Zabell S, Zumwalt
RE (2016) Forensic bitemark identification: weak foundations, exaggerated claims. Journal of
Law and the Biosciences 3(3):538-575. doi: 10.1093/jlb/lsw045.
Senn DR (2007) The good, the bad, and the ugly: A critical look at the forensic value of bite
mark analysis. Forensic Odontology News 24(6): 1, 6-9.
Sheasby DR, MacDonald DG (2001) A forensic classification of distortion in human bite marks.
Forensic Science International 122(1):75-78.
Sheets HD, Bush MA (2011) Mathematical matching of a dentition to bitemarks: use and
evaluation of affine methods. Forensic Science International 207(1-3):111-118.
Sheets HD, Bush PJ, Bush MA (2012) Bitemarks: distortion and covariation of the maxillary and
mandibular dentition as impressed in human skin. Forensic Science International 223(1-3):202-
207.
Sognnaes RF (1977) The case for better bite and bite mark preservations. International Journal
of Forensic Dentistry 4(13): 17-20.
Sognnaes RF, Rawson RD, Gratt BM, Nguyen NB (1982) Computer comparison of bitemark
patterns in identical twins. Journal of the American Dental Association 105(3):449-451.
Steadman DW, Dautartas A, Kenyhercz MW, Jantz LM, Mundorff A, Vidoli GM (2019)
Differential scavenging among pig, rabbit, and human subjects. Journal of Forensic Sciences
63(6): 1684-1691.
Stols G, Bernitz H (2010) Reconstruction of deformed bite marks using affine transformations.
Journal of Forensic Sciences 55(3):784-787.
NIST IR 8352
March 2023
33
Sweet D, Parhar M, Wood RE (1998) Computer-based production of bite mark comparison
overlays. Journal of Forensic Sciences 43(5):1050-1055.
Sweet D, Pretty I (2001) A look at forensic dentistry – Part 2: Teeth as weapons of violence –
identification of bitemark perpetrators. British Dental Journal 190(8):415-418.
Tai MW, Chong ZF, Asif MK, Rahmat RA, Nambiar P (2016) A comparative study between
xerographic, computer-assisted overlay generation and animated-superimposition methods in
bite mark analyses. Legal Medicine 22:42-48.
[TXFSC 2016] Texas Forensic Science Commission (2016) Forensic Bitemark Comparison
Complaint Filed by National Innocence Project on Behalf of Steven Mark Chaney – Final
Report. Available at https://www.txcourts.gov/media/1454500/finalbitemarkreport.pdf (1303
pages, 100 MB file). Accessed September 29, 2022.
van der Velden A, Spiessens M, Willems G (2010) Bite mark analysis and comparison using
image perception technology. Journal of Forensic Odonto-stomatology 24 (1):14-17.
Verma AK, Kumar S, Bhattacharya S (2013) Identification of a person with the help of bite mark
analysis. Journal of Oral Biology and Craniofacial Research 3(2):88-91. doi:
10.1016/j.jobcr.2013.05.002.
Vilborn P, Bernitz H (2021) A systematic review of 3D scanners and computer assisted analyzes
of bite marks: Searching for improved analysis methods during the Covid-19 pandemic.
International Journal of Legal Medicine 24:1-9.
Whittaker DK (1975) Some laboratory studies on the accuracy of bite mark comparison.
International Dental Journal 25(3):166-171.
Whittaker DK, Brickley MR, Evans L (1998) A comparison of the ability of experts and non-
experts to differentiate between adult and child human bite marks using receiver operating
characteristic (ROC) analysis. Forensic Science International 92(1):11-20.
